
An Unusual Complication of PEG Feeding After Pancreatico-Gastrostomy
Abstract
Context We describe a late complication of the pancreatico-gastrostomy (PG) anastomosis following pancreatico-duodenectomy (PD). Case report A percutaneous endoscopic gastrostomy (PEG) feeding tube was inserted many months post-operatively. In this patient activated pancreatic enzymes eroded the gastrostomy tract, resulting in pain, recurrent infection and eventual removal of the gastrostomy tube. Conclusions Where surgical insertion of a feeding jejunostomy is not viable or deemed too high risk after Whipple or PPPD, we recommend careful consideration of PEG tube insertion in patients with PG reconstruction. If a PEG is used the prophylactic use of Lanreotide is recommended.
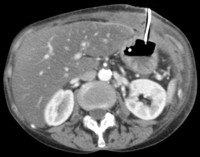
Image: CT scan following PEG-J insertion.
Downloads
References
Waugh JM, Clagett OT. Resection of the duodenum and head of the pancreas for carcinoma. An analysis of thirty cases. Surgery 1946; 20:224-32. [PMID:20994806]
Jang JY, Kim SW, Pank SJ, Park YH. Comparison of the functional outcome after pylorus preserving pancreaticoduodenectomy: Pancreatogastrostomy and pancreaticojejunostomy. World J Surg 2002; 26:366-71. [PMID:11865376]
Phillips M, Lordan JT, Menezes N, Karanjia ND. Feeding patients following pancreaticoduodenectomy: a UK national survey. Ann R Coll Surg Engl 2009; 91:385-8. [PMID:19409147]
Ganong WF. Regulations of gastrointestinal function. Review of Medical Physiology. New York: The McGraw-Hill Companies, 2005; 22:26.
Leach SD, Modlin IM, Scheele GA, Gorelick FS. Intracellular Activation of Digestive Zymogens in Rat Pancreatic Acini, The Journal of Clinical Investigation 1991; 87:362-6. [PMID:1985109]
Pikarsky AJ, Muggia-Sullam M, Eid A, Lyass S, Bloom AL, Durst AL, Shiloni E. Pancreaticogastrostomy after pancreatoduodenectomy; A retrospective study of 28 patients. Arch Surgery 1997; 132:96-299. [PMID:9125031]
Figarella C, Miszczuk-Jamska B, Barret AJ. Possible lysosomal activation of pancreatic zymogens: activation of both human trypsinogens by cathepsin B and spontaneous acid activation of human trypsinogen 1. Biol Chem Hoppe-Seyler 1998; 369:293-298. [PMID:3202969]
Ohmuraya M, Yamamura K. Autophagy and acute pancreatitis: a novel autophagy theory for trypsinogen activation. Autophagy 2008; 4:1060-1062. [PMID:18776738]
Van Acker GJ, Perides G, Steer ML. Co-localisation theory: a mechanism for the intrapancreatic activation of digestive enzymes during the early phases of acute pancreatitis. World J Gastroenterol 2006; 12:1985-90. [PMID:16610045]
Copyright (c) 2014 Mary Elizabeth Phillips, Katy Hosie, Edward J Griffiths, Nadeen Low, Michelle C Gallagher, Christopher J Tibbs, Nariman D Karanjia

This work is licensed under a Creative Commons Attribution 4.0 International License.
As a member of Publisher International Linking Association, PILA, iMedPub Group’s JOP follows the Creative Commons Attribution License and Scholars Open Access publishing policies. Journal of the Pancreas is the Council Contributor Member of Council of Science Editors (CSE) and following the CSE slogan Education, Ethics, and Evidence for Editors.