
Pancreatic Neoplasm in 2011: An Update
Abstract
Pancreatic cancer still is a significant, unresolved therapeutic challenge with nearly similar incidence and mortality rates. It is the most lethal type of digestive cancer with a 5-year survival rate of 5%. Adjuvant chemotherapy remains to be gemcitabine alone or combined with infusional 5-fluorouracil with radiation therapy. Nevertheless, only a few patients survive for at least 5 years after R0 resection and adjuvant therapy. Most patients need palliative treatment. Once pancreatic cancer becomes metastatic, it is uniformly fatal with an overall survival of typically 6 months from diagnosis. Chemotherapy is an important component of palliative care but must be administered as a part of a multidisciplinary approach, including palliation of pain, managing weight loss, and deterioration in functional status. Gemcitabine has been the standard in both locally advanced and metastatic disease. The addition of the tyrosine kinase inhibitor erlotinib prolongs median survival for only 2 weeks. While gemcitabine-based regimens are currently accepted as the standard first-line treatment of patients with locally advanced or metastatic pancreatic adenocarcinoma, there is no consensus regarding treatment in the second-line setting. It will not be untrue to say that there are no real medical breakthroughs with regards to improving the prognosis of pancreatic cancer as of 2011. On the other hand, we have made some progress in patients with advanced pancreatic neuroendocrine tumors. These patients have a 5-year survival that can range from 97% in benign insulinomas to as low as 30% in non-functional metastatic pancreatic neuroendocrine tumors. Treatment options may include surgery, transarterial chemoembolization of liver metastases, and cytotoxic therapy such as streptozotocin, 5-fluorouracil or doxorubicin. Somatostatin analogues, like octreotide, have been proven to prolong progression-free survival in patients with metastatic neuroendocrine tumors of midgut origin. In 2011, two targeted agents, a tyrosine kinase inhibitor sunitinib and mTOR inhibitor everolimus have been approved by FDA for pancreatic neuroendocrine tumors. With these approvals, U.S. physicians can now offer their patients with progressive pancreatic neuroendocrine tumors. Patients with any stage of pancreatic cancer should be considered candidates for clinical trials.
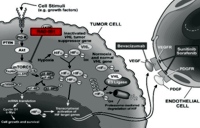
Image: Mode of action of everolimus.
Downloads
References
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010; 60:277-300.
Surveillance Epidemiology and End Results (SEER). U.S. Cancer Statistics: 1999-2007 Incidence and Mortality Report. Available at http://www.seer.cancer.gov/publications/uscs.html (Accessed January 31, 2011).
Saif MW. Controversies in the adjuvant treatment of pancreatic adenocarcinoma. JOP. J Pancreas (Online) 2007; 8:545-52.
Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985; 120:899-903.
Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R, Couvreur ML, Veenhof CH, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 1999; 230:776-82.
Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 2004; 350:1200-10.
Regine WF, Winter KA, Abrams RA, Safran H, Hoffman JP, Konski A, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA 2008; 299:1019-26.
Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA 2007; 297:267-77.
Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, et al. European Study Group for Pancreatic Cancer.Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA 2010; 304(10):1073-81.
Kim R, Saif MW. Is there an optimal neoadjuvant therapy for locally advanced pancreatic cancer? JOP. J Pancreas (Online) 2007; 8:279-88.
Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403-13.
Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25:1960-6.
Conroy T, Desseigne F, Ychou M, Ducreux M, Bouche O, Guimbaud R, et al. Randomized phase III trial comparing FOLFIRINOX (F: 5FU/leucovorin (LV), irinotecan (I), and oxaliplatin (O)) versus gemcitabine (G) as first-line treatment for metastatic pancreatic adenocarcinoma (MPA): Preplanned interim analysis results of the PRODIGE. J Clin Oncol 2010; 28(15 Suppl.):Abstract 4010.
Cunningham D, Chau I, Stocken DD, Valle JW, Smith D, Steward W, et al. Phase III randomized comparison of gemcitabine versus gemcitabine plus capecitabine in patients with advanced pancreatic cancer. J Clin Oncol 2009; 27:5513-8.
Poplin E, Feng Y, Berlin J, Rothenberg ML, Hochster H, Mitchell E, et al. Phase III, randomized study of gemcitabine and oxaliplatin versus gemcitabine (fixed-dose rate infusion) compared with gemcitabine (30-minute infusion) in patients with pancreatic carcinoma E6201: a trial of the Eastern Cooperative Oncology Group. J Clin Oncol 2009; 27:3778-85.
Kindler HL, Niedzwiecki D, Hollis D, Sutherland S, Schrag D, Hurwitz H, et al. Gemcitabine plus bevacizumab compared with gemcitabine plus placebo in patients with advanced pancreatic cancer: phase III trial of the Cancer and Leukemia Group B (CALGB 80303). J Clin Oncol 2010; 28:3617-22.
Philip PA, Goldman BH, Ramanathan RK, Lenz, Lowy AM, Whitehead RP, et al. Phase I trial of combination gemcitabine, erlotinib (NSC-718781), and IMC-A12 (NSC-742460) as first-line treatment in patients with metastatic pancreatic cancer: Southwest Oncology Group study S0727. ASCO Gastrointestinal Cancers Symposium 2010: Abstract No. 233.
Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364(19):1817-25.
Kang SP, Saif MW. Optimal second line treatment options for gemcitabine refractory advanced pancreatic cancer patients. Can we establish standard of care with available data? JOP. J Pancreas (Online) 2008; 9:83-90.
Pelzer U, Schwaner I, Stieler J, Adler M, Seraphin J, Dörken B, et al. Best supportive care (BSC) versus oxaliplatin, folinic acid and 5-fluorouracil (OFF) plus BSC in patients for second-line advanced pancreatic cancer: A phase III-study from the German CONKO-study group. Eur J Cancer. 2011 May 10. [Epub ahead of print]
Saif MW. Is there a standard of care for the management of advanced pancreatic cancer? Highlights from the Gastrointestinal Cancers Symposium. Orlando, FL, USA. January 25-27, 2008. JOP. J Pancreas (Online) 2008; 9:91-8.
Ramage JK, Davies AHG, Ardill et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours. Gut 2005; 54:iv1-16
Halfdanarson TR, Rabe KG, Rubin J, Petersen GM. Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Ann Oncol 2008; 19:1727-33.
Ehehalt F, Saeger HD, Schmidt CM, Grützmann R. Neuroendocrine tumors of the pancreas. Oncologist 2009; 14:456-67.
Franko J, Feng W, Yip L, Genovese E, Moser AJ. Non-functional neuroendocrine carcinoma of the P pancreas: incidence, tumor biology, and outcomes in 2,158 patients. J Gastrointest Surg 2010; 14:541-8.
Halfdanarson TR, Rabe KG, Rubin J, Petersen GM. Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Ann Oncol 2008; 19:1727-33.
Liu DM, Kennedy A, Turner D, Rose SC, Kee ST, Whiting S, et al. Minimally invasive techniques in management of hepatic neuroendocrine metastatic disease. Am J Clin Oncol 2009; 32:200-15.
Hill JS, McPhee JT, McDade TP, Zhou Z, Sullivan ME, Whalen GF, Tseng JF. Pancreatic neuroendocrine tumors: the impact of surgical resection on survival. Cancer 2009; 115:741-51.
Moertel CG, Lefkopoulo M, Lipsitz S, Hahn RG, Klaassen D. Streptozocin-doxorubicin, streptozocin-fluorouracil or chlorozotocin in the treatment of advanced islet-cell carcinoma. N Engl J Med 1992; 326:519-23.
Kouvaraki MA, Ajani JA, Hoff P, Wolff R, Evans DB, Lozano R, Yao JC. Fluorouracil, doxorubicin, and streptozocin in the treatment of patients with locally advanced and metastatic pancreatic endocrine carcinomas. J Clin Oncol 2004; 22:4762-71.
Ramanathan RK, Cnaan A, Hahn RG, Carbone PP, Haller DG. Phase II trial of dacarbazine (DTIC) in advanced pancreatic islet cell carcinoma. Study of the Eastern Cooperative Oncology Group-E6282. Ann Oncol 2001; 12:1139-43.
Arnold R, Müller H, Schade-Brittinger C, Rinke A, Klose K, Barth P, et al. Placebo-controlled, double-blind, prospective, randomized study of the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID study group. J Clin Oncol 2009; 27(Suppl):4508.
Raymond E, Dahan L, Raoul JL, Bang YJ, Borbath I, Lombard-Bohas C, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:501-13.
Yao JC, Shah MH, Ito T, Bohas CL, Wolin EM, Van Cutsem E, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Eng J Med 2011; 364:514-23.
Saif MW. Pancreatic cancer: is this bleak landscape finally changing? Highlights from the '43rd ASCO Annual Meeting'. Chicago, IL, USA. June 1-5, 2007. JOP. J Pancreas (Online) 2007; 8:365-73.
Hardacre JM, Mulcahy MF, Small W Jr, Talamonti M, Obel JC, Rocha Lima CS, et al. Effect of the addition of algenpantucel-L immunotherapy to standard adjuvant therapy on survival in patients with resected pancreas cancer. J Clin Oncol 2011; 29(Suppl. 4):236.
Pharmaceutical International's Research Correspondent. Phase III TeloVac cancer vaccine trials underway. Pharmaceutical International News 2011; April.
Rini BI, Campbell SC, Escudier B. Renal cell carcinoma. Lancet 2009 Mar 28; 373(9669):1119-32. Epub 2009 Mar 5.
Copyright (c) 2011 Muhammad Wasif Saif

This work is licensed under a Creative Commons Attribution 4.0 International License.
As a member of Publisher International Linking Association, PILA, iMedPub Group’s JOP follows the Creative Commons Attribution License and Scholars Open Access publishing policies. Journal of the Pancreas is the Council Contributor Member of Council of Science Editors (CSE) and following the CSE slogan Education, Ethics, and Evidence for Editors.