
Disconnected Duct Syndrome: Refractory Inflammatory External Pancreatic Fistula Following Percutaneous Drainage of an Infected Peripancreatic Fluid Collection. A Case Report and Review of the Literature
Abstract
Context Inflammatory external pancreatic fistulas behave differently from postoperative external pancreatic fistulas in that the former are less likely to close without intervention and take a longer time to do so. The principal determinants of closure of an external pancreatic fistula are the anatomy of the fistulous tract (end versus side, main duct versus side branch), the presence of downstream ductal obstruction, ongoing peripancreatic inflammation and etiology of the fistula (inflammatory versus postoperative). While the approach to diagnosis and management of postoperative pancreatic fistulas has been standardized, the same is lacking for inflammatory external pancreatic fistulas, partly due to the absence of a unifying definition of the latter and a paucity of data on the topic. Case report We report the case of disconnected duct syndrome, an end inflammatory fistula, following percutaneous drainage of an infected pancreatic fluid collection with two failed attempts at endoscopic treatment, treated successfully by surgery, and we also attempted to review the literature on the topic. Conclusions “Disconnected duct syndrome”, an end inflammatory fistula, following percutaneous or surgical treatment of severe acute pancreatitis is a distinct entity as spontaneous closure is exceedingly uncommon. Surgery is almost always required and is successful in the majority of cases.
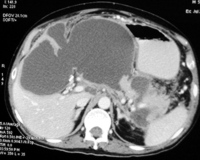
Image: CECT abdomen showing a large intrapancreatic fluid collection extending into the hepatogastric ligament.
Downloads
References
Paloyan D, Simonowitz D, Blackstone M. Pancreatic fistula: management guided by endoscopic retrograde cholangiopancreatography. Arch Surg 1977; 112:1139-40. [PMID 901188]
Miller BM, Traverso LW, Freeny PC, Abumrad NN. Failure of somatostatin or an analog to promote closure of end pancreatic fistulae. Int J Pancreatol 1989; 4:65-72. [PMID 2466917]
Prinz RA, Pickleman J, Hoffman JP. Treatment of pancreatic cutaneous fistulas with a somatostatin analog. Am J Surg 1988; 155:36-42. [PMID 2893556]
Voss M, Ali A, Eubanks WS, Pappas TN. Surgical management of pancreaticocutaneous fistula. J Gastrointest Surg 2003; 7:542-6. [PMID 12763413]
Alexakis N, Sutton R, Neoptolemos JP. Surgical treatment of pancreatic fistula. Dig Surg 2004; 21:262-74. [PMID 15308865]
Howard TJ, Stonerock CE, Sarkar J, Lehman GA, Sherman S, Wiebke EA, et al. Contemporary treatment strategies for external pancreatic fistulas. Surgery 1998; 124:627-32. [PMID 9780981]
Howard TJ, Rhodes GJ, Selzer DJ, Sherman S, Fogel E, Lehman GA. Roux-en-Y internal drainage is the best surgical option to treat patients with disconnected duct syndrome after severe acute pancreatitis. Surgery 2001; 130:714-21. [PMID 11602903]
Sandrasegaran K, Tann M, Jennings SG, Maglinte DD, Peter SD, Sherman S, Howard TJ. Disconnection of the pancreatic duct: an important but overlooked complication of severe acute pancreatitis. Radiographics 2007; 27:1389-1400. [PMID 17848698]
Akisik MF, Sandrasegaran K, Aisen AA, Maglinte DD, Sherman S, Lehman GA. Dynamic secretin-enhanced MR cholangiopancreatography. Radiographics 2006; 26:665-77. [PMID 16702446]
Nair RR, Lowy AM, McIntyre B, Sussman JJ, Matthews JB, Ahmad SA. Fistulojejunostomy for the management of refractory pancreatic fistula. Surgery 2007; 142:636-42. [PMID 17950358]
Findeiss LK, Brandabur J, Traverso LW, Robinson DH. Percutaneous embolization of the pancreatic duct with cyanoacrylate tissue adhesive in disconnected duct syndrome. J Vasc Interv Radiol 2003; 14:107-11. [PMID 12525595]
Bassi C, Butturini G, Salvia R, Contro C, Valerio A, Falconi M, Pederzoli P. A single-institution experience with fistulojejunostomy for external pancreatic fistulas. Am J Surg 2000; 179:203-6. [PMID 10827321]
Lawrence C, Howell DA, Stefan AM, Conklin DE, Lukens FJ, Martin RF, et al. Disconnected pancreatic tail syndrome: potential for endoscopic therapy and results of long-term follow-up. Gastrointest Endosc 2008; 67:673-9. [PMID 18054008]
Pelaez-Luna M, Vege SS, Petersen BT, Chari ST, Clain JE, Levy MJ, et.al. Disconnected pancreatic duct syndrome in severe acute pancreatitis: clinical and imaging characteristics and outcomes in a cohort of 31 cases. Gastrointest Endosc 2008; 68: 91-7. [PMID 18378234]
Varadarajulu S, Noone TC, Tutuian R, Hawes RH, Cotton PB. Predictors of outcome in pancreatic duct disruption managed by endoscopic transpapillary stent placement. Gastrointest Endosc 2005; 61:568-75. [PMID 15812410]
Copyright (c) 2011 Rashesh Solanki, Suman Bhushan Koganti, Nagari Bheerappa, Regulagedda Adikeshava Sastry

This work is licensed under a Creative Commons Attribution 4.0 International License.
As a member of Publisher International Linking Association, PILA, iMedPub Group’s JOP follows the Creative Commons Attribution License and Scholars Open Access publishing policies. Journal of the Pancreas is the Council Contributor Member of Council of Science Editors (CSE) and following the CSE slogan Education, Ethics, and Evidence for Editors.